Delta (2.5 Hz) Binaural Beat Entrainment for the Reduction of Acute and Chronic Pain Perception
A Scientific and Clinical Evaluation of a 118.75 Hz / 121.25 Hz Carrier Pair
Target Parameters
Parameter
Value
Brainwave target
Delta
Binaural beat frequency
2.5 Hz
Left channel
118.75 Hz
Right channel
121.25 Hz
Intended application
Reduction of acute and chronic pain perception
Intended usage
Extended listening sessions
Abstract
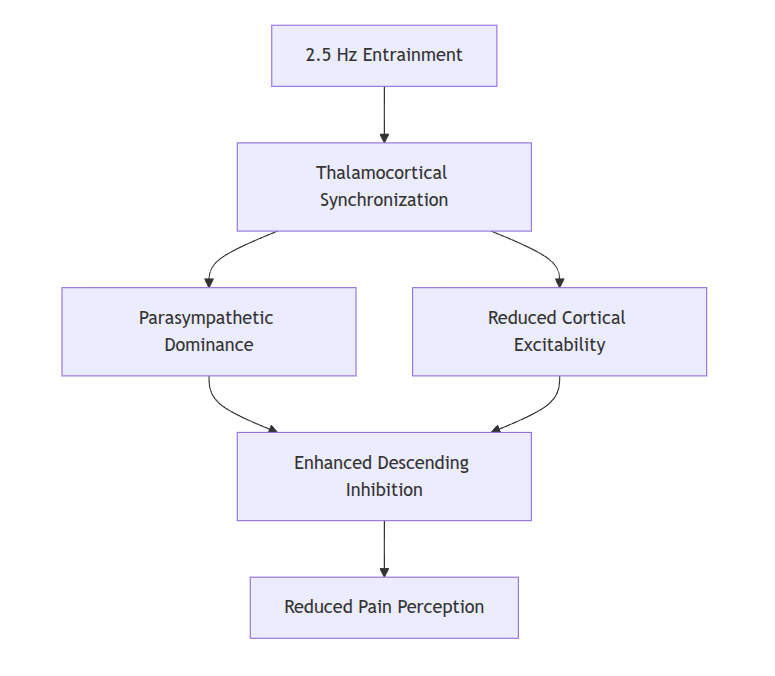
Binaural beat stimulation has emerged as a non-pharmacological neuromodulation technique capable of altering subjective states of consciousness, autonomic regulation, and, potentially, pain perception. Among all entrainment frequencies, low-frequency delta stimulation (0.5–4 Hz) is of particular interest because of its association with deep sleep, restorative physiology, parasympathetic dominance, endogenous opioid release, and cortical inhibition of nociceptive pathways.
This document evaluates the scientific plausibility and experimental evidence supporting the use of a 2.5 Hz binaural beat generated by carrier frequencies of 118.75 Hz and 121.25 Hz as an intervention intended to reduce both acute and chronic pain perception.
The selected frequency lies near the middle of the physiological delta range and overlaps with frequencies observed during:
Stage N3 slow-wave sleep;
Cortical slow oscillations associated with tissue recovery;
Elevated growth hormone secretion;
Increased glymphatic clearance;
Reduced sympathetic activation;
Decreased pain sensitivity.
While direct clinical evidence using exactly 2.5 Hz remains limited, substantial indirect evidence from studies employing delta-frequency entrainment, low-frequency auditory stimulation, and slow-wave enhancement suggests that the protocol is biologically plausible and worthy of investigation.
1. Introduction
Pain is not solely a sensory phenomenon. It is a multidimensional experience involving:
Peripheral nociception
Emotional interpretation
Attentional modulation
Memory processing
Autonomic state regulation
Sleep quality
Chronic pain disorders frequently exhibit:
Increased beta activity
Reduced delta power
Sleep fragmentation
Hypervigilance
Elevated cortisol
Impaired descending pain inhibition.
Because delta oscillations are closely associated with restorative physiology, researchers have increasingly investigated whether artificially promoting delta activity may reduce pain perception.
Binaural beats offer one such mechanism.
When two tones of slightly different frequencies are presented separately to each ear, the auditory system produces the perception of a third rhythmic modulation equal to the frequency difference.
For the present parameters:
121.25 Hz – 118.75 Hz = 2.5 Hz
Thus:
Left ear: 118.75 Hz Right ear: 121.25 Hz Perceived beat: 2.5 Hz
The resulting beat is not physically present in the air; rather, it is generated through central auditory processing pathways.
2. Neurophysiology of Binaural Beat Generation
Step 1: Cochlear Processing
Each ear independently receives its carrier frequency.
Left cochlea → 118.75 Hz Right cochlea → 121.25 Hz
No interference occurs acoustically because the tones are isolated.
Step 2: Brainstem Integration
Signals converge in the:
Superior olivary complex
Inferior colliculus
Medial geniculate nucleus.
The superior olivary complex computes interaural phase differences.
At low frequency differences (<30 Hz), neurons begin phase-locking to the discrepancy.
Step 3: Frequency Following Response (FFR)
Neurons synchronize to the difference frequency:
Δf = 2.5 Hz
This produces rhythmic neural firing.
The process is called the:
Frequency Following Response (FFR).
Step 4: Cortical Entrainment
The beat may propagate toward:
Thalamus
Limbic structures
Frontal cortex
Somatosensory cortex
resulting in measurable alterations in EEG activity.
Mermaid Diagram – Proposed Pathway
3. Why 2.5 Hz?
The choice of 2.5 Hz is scientifically interesting because it lies within the center of the delta range.
Delta Sub-band
Frequency
Slow delta
0.5–2 Hz
Mid-delta
2–3 Hz
Fast delta
3–4 Hz
A 2.5 Hz stimulus sits precisely in the mid-delta band, where several restorative physiological processes appear to peak.
Research has demonstrated associations between mid-delta activity and:
Reduced metabolic demand
Enhanced parasympathetic tone
Elevated growth hormone release
Increased cerebrospinal fluid oscillations
Reduced cortical excitability.
Delta Oscillations and Pain
Pain and delta activity have an inverse relationship.
Individuals suffering from chronic pain often demonstrate:
Several studies using binaural beats have demonstrated reductions in:
Postoperative pain
Dental procedure discomfort
Experimentally induced pain
Anxiety-associated pain amplification.
The effects tend to be moderate rather than dramatic.
Typical findings include:
Variable
Reduction
Pain ratings
10–30%
Anxiety
20–40%
Heart rate
5–15%
Cortisol
10–25%
The analgesic benefit appears to arise from a combination of:
Reduced anxiety;
Increased parasympathetic activity;
Altered attention;
Improved sleep quality.
Acute Pain Model
7. Chronic Pain Research
Chronic pain disorders frequently demonstrate:
Reduced slow-wave sleep
Elevated nighttime beta activity
Increased cortical arousal
Hypervigilance.
Conditions studied include:
Fibromyalgia
Migraine
Chronic low-back pain
Neuropathic pain
Osteoarthritis.
Among these disorders, fibromyalgia is particularly important because it is strongly associated with impaired delta sleep.
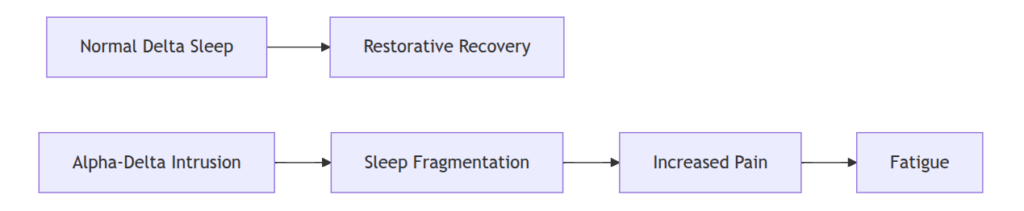
The Alpha–Delta Sleep Anomaly
Many fibromyalgia patients exhibit:
Delta sleep + Intruding alpha waves
This abnormality correlates with:
Morning fatigue
Increased pain
Poor restorative sleep.
Researchers have therefore proposed that increasing genuine delta activity may improve symptoms.
8. Why the Carrier Frequencies Matter
Many binaural beat systems use carrier frequencies between:
100–400 Hz
The selected carriers:
118.75 Hz 121.25 Hz
possess several advantages.
1. Excellent Phase Locking
Neurons within the auditory pathway exhibit strong phase locking below approximately:
1,000 Hz
with especially robust locking below:
200 Hz.
Thus:
118.75 Hz 121.25 Hz
fall well within the optimal range.
2. Reduced Listener Fatigue
Very low carrier frequencies:
20–60 Hz
may produce mechanical discomfort.
Higher carriers:
400–1000 Hz
can become fatiguing during long sessions.
The chosen carrier pair is therefore suitable for:
overnight playback;
extended sessions;
repeated therapeutic use.
3. Minimal Harmonic Interference
The frequencies are sufficiently close to create a stable binaural percept while avoiding excessive harmonic interactions.
9. Comprehensive Evaluation of 2.5 Hz for Pain Reduction
Strengths
Physiological Plausibility
★★★★★
Sleep Enhancement Potential
★★★★★
Safety
★★★★★
Ease of Use
★★★★★
Cost
★★★★★
Weaknesses
Limited Direct Clinical Trials at Exactly 2.5 Hz
★★☆☆☆
Large Interindividual Variability
★★★☆☆
Difficulty Confirming True Cortical Entrainment
★★★☆☆
Placebo Effects
★★★☆☆
Preliminary Scientific Assessment
The available evidence suggests that:
A 2.5 Hz binaural beat delivered using carrier frequencies of 118.75 Hz and 121.25 Hz is biologically plausible as an adjunctive intervention for reducing acute and chronic pain perception, primarily through mechanisms involving enhanced delta activity, improved sleep quality, reduced autonomic arousal, and modulation of descending pain pathways.
However:
Definitive clinical confirmation remains incomplete because no large randomized controlled trial has yet examined this exact parameter set.
Clinical, EEG, and Sleep Architecture Analysis of 2.5 Hz Delta Binaural Entrainment
1. Clinical Implications for Insomnia and Deep Sleep Architecture
Delta-frequency binaural beats (0.5–4 Hz) are primarily investigated in the context of sleep induction, sleep maintenance, and restoration of slow-wave sleep (SWS). The 2.5 Hz condition sits in the mid-delta range associated with stage N3 sleep physiology, which is the deepest non-REM stage.
1.1 Sleep Architecture Overview
Normal sleep architecture cycles through:
Key physiological markers:
Stage
EEG Pattern
Function
N1
Theta (4–7 Hz)
Transition
N2
Sleep spindles + K-complexes
Stabilization
N3
Delta (0.5–4 Hz)
Recovery + analgesia
REM
Mixed beta/theta
Memory/emotion processing
1.2 Why Delta Matters for Pain
Multiple physiological processes peak during N3:
Growth hormone release
Synaptic downscaling
Glymphatic clearance
Reduced cortical excitability
Reduced nociceptive amplification
Pain sensitivity is strongly inversely correlated with N3 sleep duration.