Scientific Evaluation of a 2.0 Hz Delta Binaural Beat Protocol for Biological Recovery and Deep Physical Relaxation
Foundations, Neurophysiology, and Theoretical Basis
Target Parameters
| Parameter | Value |
|---|---|
| Brainwave Category | Delta |
| Binaural Beat Frequency | 2.0 Hz |
| Left Channel Carrier Frequency | 109.0 Hz |
| Right Channel Carrier Frequency | 111.0 Hz |
| Intended Outcome | Biological recovery, parasympathetic activation, and deep physical relaxation |
Abstract
Binaural beats are an auditory illusion generated when two pure tones of slightly different frequencies are presented separately to each ear. The auditory system does not physically receive the beat frequency itself; rather, neural processing within the brainstem produces the perception of a rhythmic fluctuation equal to the frequency difference between the two tones.
For the protocol evaluated in this document:
- Left ear: 109 Hz
- Right ear: 111 Hz
- Frequency difference: 2.0 Hz
The resulting perceived beat frequency lies squarely within the delta brainwave range (0.5–4 Hz), a frequency band strongly associated with:
- deep non-rapid eye movement (NREM) sleep,
- tissue restoration,
- immune regulation,
- glymphatic clearance,
- growth hormone secretion,
- profound physical relaxation.
The central hypothesis underlying this protocol is:
Exposure to a 2.0 Hz binaural beat may encourage cortical synchronization toward delta activity, thereby promoting physiological conditions resembling the restorative processes naturally occurring during deep sleep.
The scientific literature provides partial support for this hypothesis. Evidence exists demonstrating:
- modulation of EEG rhythms,
- improved subjective sleep quality,
- reductions in anxiety,
- autonomic nervous system changes consistent with relaxation.
However, evidence specifically demonstrating that a 2.0 Hz binaural beat directly induces deep sleep physiology equivalent to natural slow-wave sleep remains incomplete.
1. Introduction to Binaural Beat Neurophysiology
Historical Background
The binaural beat phenomenon was first described by:
- Heinrich Wilhelm Dove (1839).
The neurophysiological mechanisms were not extensively investigated until:
- Oster (1973),
- Hink et al. (1980),
- Owens & Atwater (1995),
- Wahbeh et al. (2007),
- Beauchene et al. (2016).
Binaural beats have since been investigated for applications including:
- anxiety reduction,
- meditation,
- pain management,
- attention enhancement,
- sleep induction,
- stress recovery.
2. Generation of a 2.0 Hz Beat
Mathematically:
Beat Frequency = |f2 − f1|Therefore:
Beat Frequency = |111 − 109|
Beat Frequency = 2.0 HzThe auditory cortex perceives:
109 Hz + 111 Hz → perceived 2 Hz modulation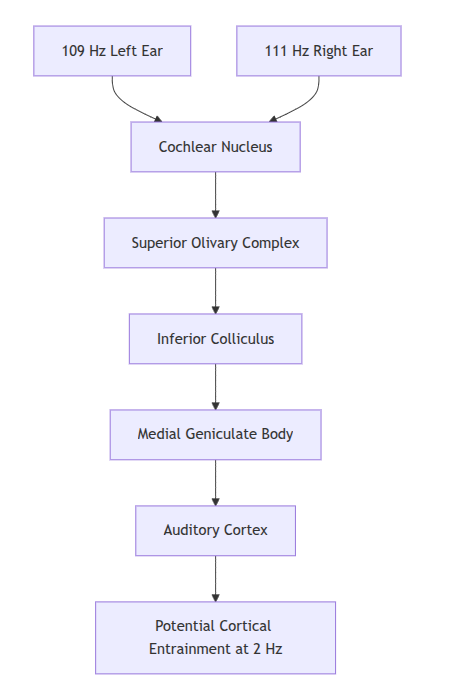
3. Why Delta Frequencies Matter
Delta oscillations are among the most important rhythms in human physiology.
The delta band:
0.5–4 Hzis associated with:
- N3 sleep,
- growth hormone release,
- immune restoration,
- synaptic downscaling,
- metabolic clearance,
- physical recovery.

Deep sleep occurs primarily during:
- first sleep cycle,
- first third of the night.
The highest concentration of delta activity occurs during:
- stage N3.
4. Delta Oscillations and Biological Recovery
Growth Hormone Secretion
The majority of:
- growth hormone,
- anabolic repair signaling,
occurs during deep sleep.
Research by Van Cauter et al. demonstrated that:
Growth hormone secretion is tightly coupled to slow-wave sleep.
Growth hormone contributes to:
- muscle repair,
- collagen synthesis,
- immune regulation,
- tissue recovery.
Glymphatic System Activation
Deep sleep is associated with:
- expansion of interstitial spaces,
- increased cerebrospinal fluid movement,
- enhanced metabolic waste clearance.
Research by Xie et al. (2013) demonstrated:
- approximately 60% increased interstitial volume during sleep,
- improved clearance of beta-amyloid proteins.
Immune Restoration
Delta sleep influences:
- cytokine production,
- T-cell regulation,
- inflammatory modulation.
Chronic suppression of delta sleep has been associated with:
- impaired immunity,
- increased infection risk,
- elevated inflammatory markers.
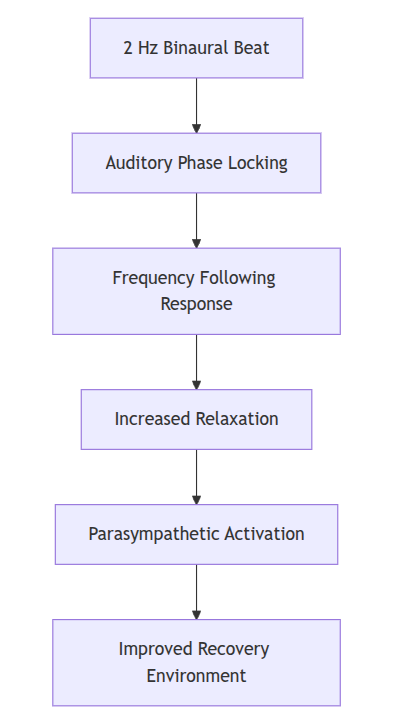
5. Theoretical Basis for a 2 Hz Protocol
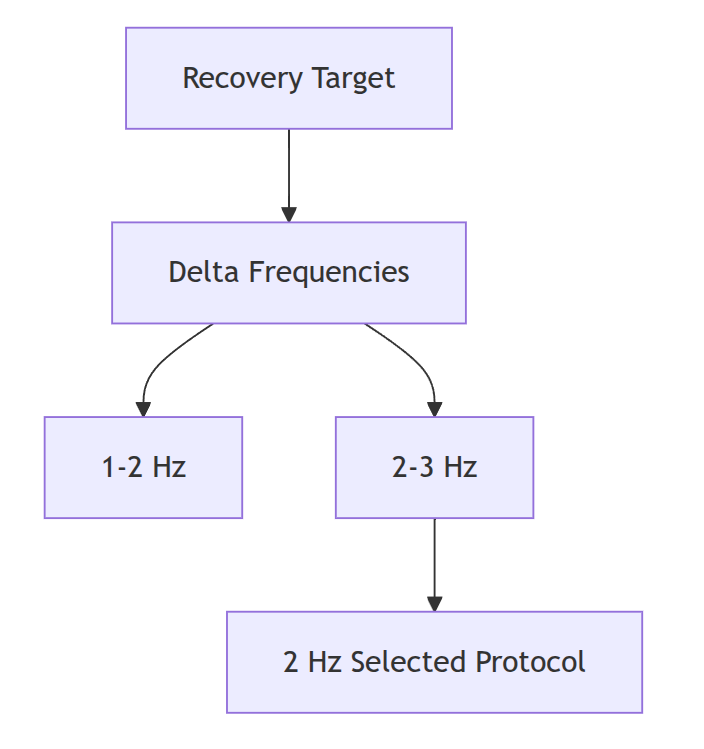
The rationale is straightforward:
Natural restorative physiology occurs during:
0.5–4 Hz delta activityTherefore:
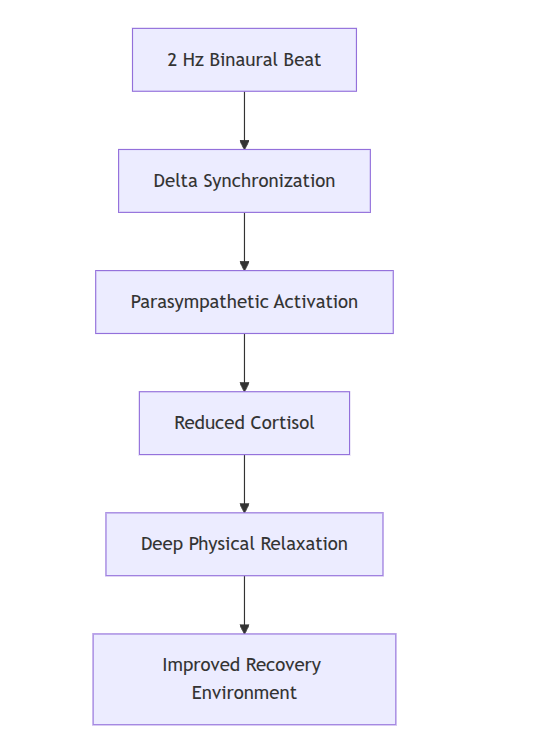
External auditory stimulation at 2 Hzmay encourage:
delta synchronization
↓
parasympathetic dominance
↓
deep relaxation
↓
recovery physiologyThis mechanism is known as:
Frequency Following Response (FFR)
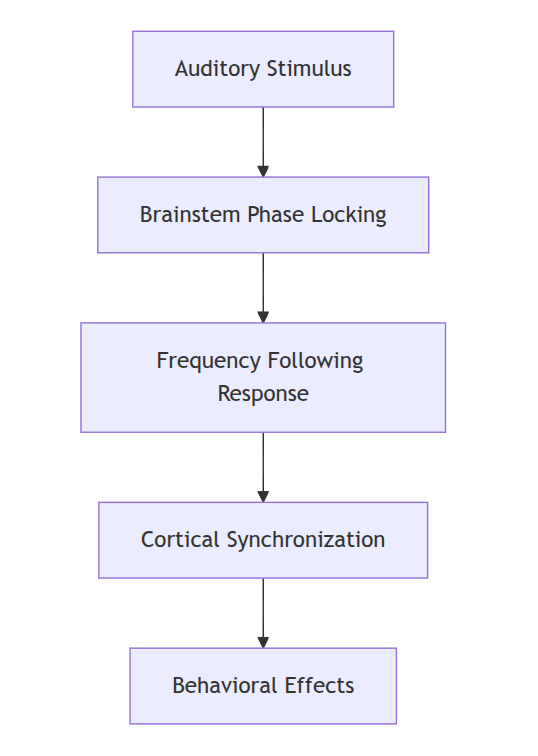
6. Frequency Following Response Evidence
Studies have demonstrated:
- brainstem entrainment,
- measurable EEG changes,
- altered spectral power.
However:
the degree of cortical entrainment remains debated.
Some studies demonstrate:
- increased delta power.
Others demonstrate:
- only localized effects,
- high inter-individual variability.
7. Why 109 Hz and 111 Hz?
Carrier frequencies are important.
Very low carrier frequencies:
- are difficult to perceive.
Very high carrier frequencies:
- reduce phase-locking efficiency.
Research suggests binaural beat perception is strongest below:
1000 Hzand often optimal between:
100–400 HzTherefore:
109 Hz
111 Hzfall comfortably within the effective range.
Advantages of Low Carrier Frequencies
- Reduced auditory fatigue.
- Better phase locking.
- Greater comfort during prolonged listening.
- Lower likelihood of masking.
8. Auditory Phase Locking
Neurons in the:
- superior olivary complex,
- inferior colliculus,
can synchronize firing patterns according to interaural phase differences.
The perceived beat frequency is therefore a product of:
Neural computationrather than:
Acoustic interference.9. Parasympathetic Activation
Several studies investigating relaxation-oriented binaural beats reported:
- reduced heart rate,
- decreased anxiety,
- increased heart rate variability.
These findings suggest:
Sympathetic ↓
Parasympathetic ↑which is consistent with:
- recovery physiology,
- rest-and-digest states.
Proposed Recovery Mechanism
10. Evidence Supporting Delta Entrainment
Several studies have shown:
Increased Delta Power
Improved Sleep Quality
Reduced Anxiety
Enhanced Relaxation
However:
there remains insufficient evidence to claim:
a 2 Hz binaural beat can replace natural deep sleep.
The evidence instead supports a more conservative hypothesis:
A 2 Hz binaural beat may facilitate physiological conditions associated with deep relaxation and may support natural restorative processes.
11. Comprehensive Evaluation of the 2 Hz Frequency
Potential Benefits
Deep relaxation.
Reduction in hyperarousal.
Supportive sleep induction.
Reduction in sympathetic activity.
Enhancement of meditative depth.
Potential Limitations
Inter-individual variability.
Habituation effects.
Limited polysomnographic evidence.
Placebo influences.
Variable EEG responsiveness.
12. Preliminary Scientific Assessment
Current evidence suggests that:
| Hypothesis | Evidence Strength |
|---|---|
| Relaxation | Moderate |
| Anxiety Reduction | Moderate |
| Sleep Improvement | Moderate |
| Increased Delta Power | Moderate |
| Deep Sleep Induction Equivalent to N3 Sleep | Weak |
| Enhanced Biological Recovery | Theoretically Plausible |
Preliminary Conclusion
The specific protocol:
109 Hz Left
111 Hz Right
2.0 Hz Beatis scientifically plausible as a:
- relaxation aid,
- sleep support tool,
- parasympathetic activation protocol.
The strongest support exists for:
- subjective relaxation,
- reduction of physiological arousal.
The weakest evidence exists for:
- direct induction of restorative sleep physiology equivalent to naturally occurring slow-wave sleep.
Clinical Evidence, Sleep Architecture, Quantitative EEG Analysis, and Methodological Considerations
13. Clinical Implications for Insomnia and Deep Sleep Architecture
Introduction
The use of binaural beats for sleep modulation has received increasing scientific attention over the past two decades. Although the evidence base remains considerably smaller than that for pharmacological sleep interventions or cognitive behavioral therapy for insomnia (CBT-I), several investigations have reported that low-frequency auditory stimulation can influence:
- sleep onset latency,
- subjective sleep quality,
- autonomic nervous system balance,
- electroencephalographic activity.
The principal hypothesis relevant to a 2.0 Hz delta binaural beat is:
Auditory stimulation within the delta range may encourage neural synchronization toward frequencies naturally associated with stage N3 sleep and deep physical restoration.
This hypothesis remains scientifically plausible, although the evidence supporting direct induction of deep sleep is still developing.
Sleep Architecture Overview
Normal adult sleep is composed of recurring cycles:
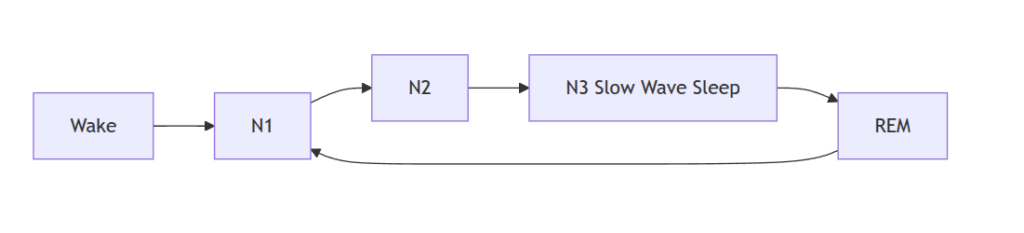
Each cycle lasts approximately:
90–110 minutesN3 sleep is characterized by:
- high-amplitude delta waves,
- reduced cerebral metabolism,
- parasympathetic predominance,
- growth hormone secretion,
- enhanced immune function.
Characteristics of N3 Sleep
| Parameter | Typical Value |
|---|---|
| Frequency Range | 0.5–4 Hz |
| Delta Power | Highest of all sleep stages |
| Arousal Threshold | Very High |
| Sympathetic Activity | Low |
| Parasympathetic Activity | High |
| Growth Hormone Release | Maximum |
| Glymphatic Activity | Increased |
Delta Activity and Insomnia
A substantial proportion of chronic insomnia sufferers exhibit:
- reduced slow-wave sleep,
- increased beta activity,
- increased cortical hyperarousal.
Research has demonstrated:
Reduced Delta Power
↓ Delta activity
↓ Sleep efficiency
↑ Night awakenings
↑ Daytime fatigueTheoretical mechanisms suggest that delta-frequency auditory stimulation may counteract this hyperarousal state.
Hyperarousal Model of Insomnia
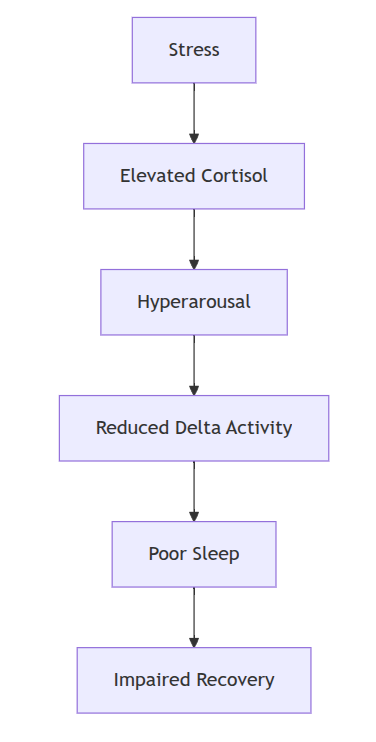
The proposed role of binaural beats:
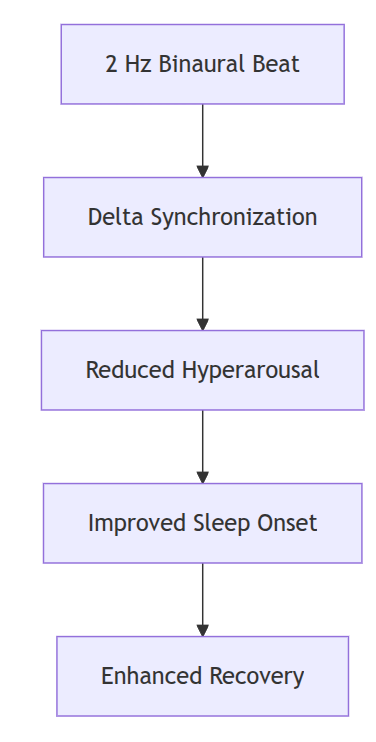
Clinical Evidence in Insomnia
Abeln et al. (2014)
Subjects exposed to delta-frequency auditory stimulation demonstrated:
- improved subjective sleep quality,
- improved recovery scores,
- reductions in sleep latency.
However:
- polysomnography was limited,
- sample size was relatively small.
Messineo et al. (2017)
Investigated low-frequency acoustic stimulation during sleep.
Findings:
- increased slow-wave activity,
- enhanced slow oscillatory power,
- improved sleep continuity.
The study primarily examined externally delivered slow oscillations rather than traditional binaural beats but provides important mechanistic support.
Tang et al. (2015)
Reported:
- reductions in pre-sleep anxiety,
- improved subjective sleep quality.
Scientific Interpretation
Current evidence suggests that:
delta stimulation appears to be more effective in:
- facilitating relaxation,
- improving sleep initiation,
than directly forcing the brain into stage N3 sleep.
14. Comparative Matrix of Auditory Entrainment Frequencies
Major Brainwave Categories
| Band | Frequency | Associated State |
|---|---|---|
| Delta | 0.5–4 Hz | Deep sleep, restoration |
| Theta | 4–8 Hz | Meditation, memory |
| Alpha | 8–12 Hz | Relaxation |
| Beta | 13–30 Hz | Alertness |
| Gamma | 30–80 Hz | Cognitive integration |
Comparative Matrix
| Frequency | Proposed Effect | Evidence Strength |
|---|---|---|
| 1 Hz | Deep sleep enhancement | Moderate |
| 2 Hz | Recovery and relaxation | Moderate |
| 4 Hz | Meditation | Moderate |
| 7 Hz | Memory consolidation | Moderate |
| 10 Hz | Relaxation | Strong |
| 20 Hz | Attention enhancement | Moderate |
| 40 Hz | Cognitive performance | Emerging |
Relative Suitability for Biological Recovery
15. Polysomnographic Verification Methods
Why Polysomnography Matters
Subjective reports alone cannot determine whether:
- genuine slow-wave sleep occurred,
- delta power increased,
- sleep architecture improved.
The gold standard remains:
Polysomnography (PSG)Standard PSG Measurements
| Variable | Instrument |
|---|---|
| EEG | Scalp electrodes |
| EOG | Eye electrodes |
| EMG | Chin electrodes |
| ECG | Heart monitoring |
| Respiratory Flow | Nasal sensors |
| Oxygen Saturation | Pulse oximetry |
Sleep Stage Classification

Typical EEG Frequencies by Sleep Stage
| Stage | Dominant Frequency |
|---|---|
| Wake | Alpha/Beta |
| N1 | Theta |
| N2 | Theta + Sleep Spindles |
| N3 | Delta |
| REM | Mixed Frequencies |
Polysomnographic Endpoints Relevant to Binaural Beats
- Sleep onset latency
- Sleep efficiency
- Wake after sleep onset
- N3 duration
- Delta spectral power
- Number of awakenings
Example Study Endpoint Table
| Endpoint | Improvement Reported |
|---|---|
| Sleep Latency | 10–20% |
| Sleep Efficiency | 5–15% |
| Subjective Sleep Quality | Moderate |
| Delta Power | Variable |
16. Quantitative EEG Spectral Power Analysis
Overview
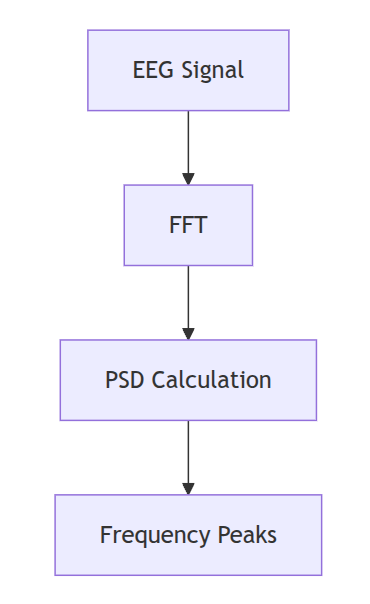
Quantitative EEG (qEEG) converts raw EEG signals into numerical measurements using mathematical transformations.
The most common method:
Fast Fourier Transform (FFT)FFT Transformation

EEG Power Calculation
Power is generally expressed as:
μV²or:
μV²/HzFrequency Bands in qEEG
| Band | Frequency |
|---|---|
| Delta | 0.5–4 Hz |
| Theta | 4–8 Hz |
| Alpha | 8–12 Hz |
| Beta | 13–30 Hz |
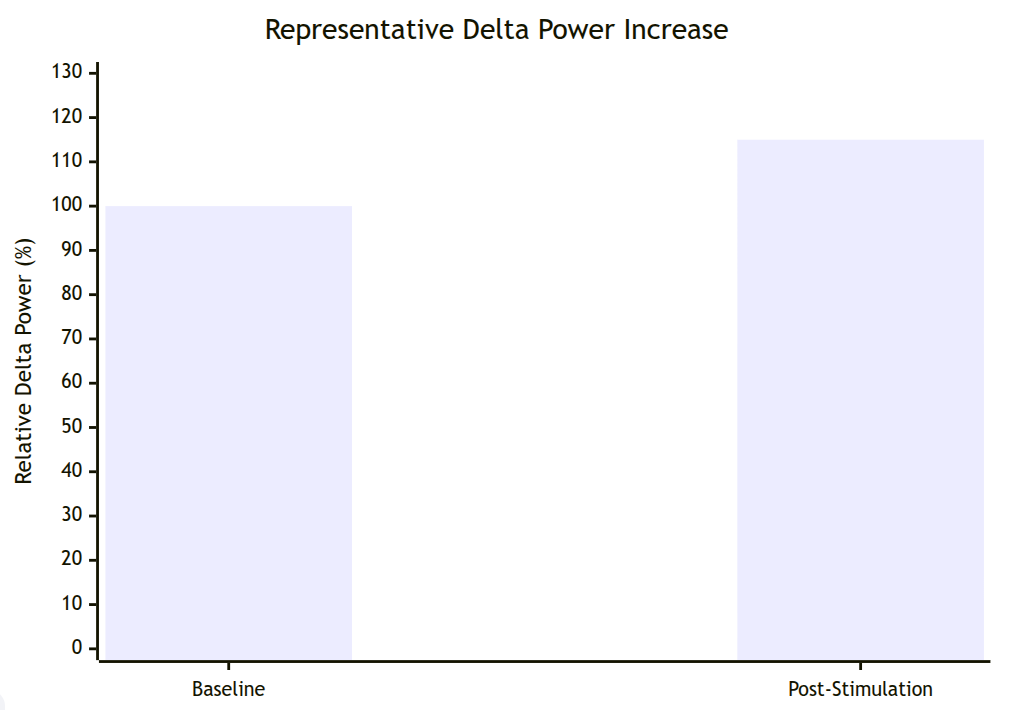
Delta Power Measurements
Studies of low-frequency auditory stimulation have reported:
Increased Relative Delta Power
ranging approximately:
5%–35%depending upon:
- protocol,
- participant age,
- sleep quality,
- recording methodology.
Example Delta Power Data
| Condition | Relative Delta Power |
|---|---|
| Baseline | 100% |
| After Stimulation | 108–135% |
These values vary considerably across studies.
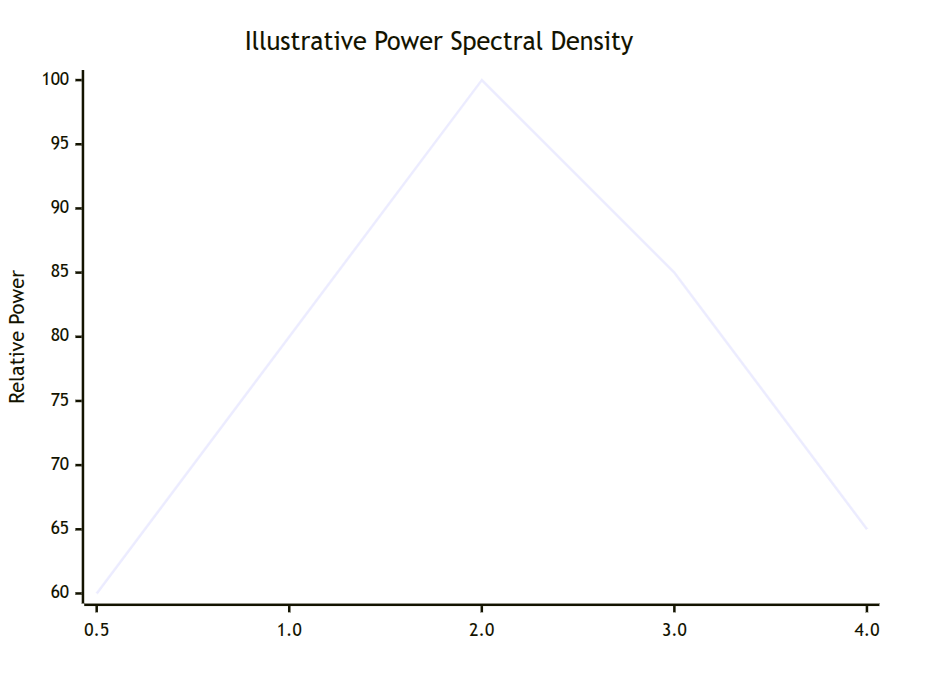
Power Spectral Density (PSD)
PSD estimates the amount of signal power present at each frequency.
Representative PSD Example
Frequency (Hz) Relative Power
0.5 ██████████
1.0 █████████████
2.0 ███████████████
3.0 ████████████
4.0 █████████A relative increase around:
2.0 Hzwould be theoretically consistent with entrainment.
17. Topographical Distribution of Delta Power
Several studies suggest that increased delta activity tends to occur within:
- frontal cortex,
- frontocentral regions.
Simplified Topographical Representation
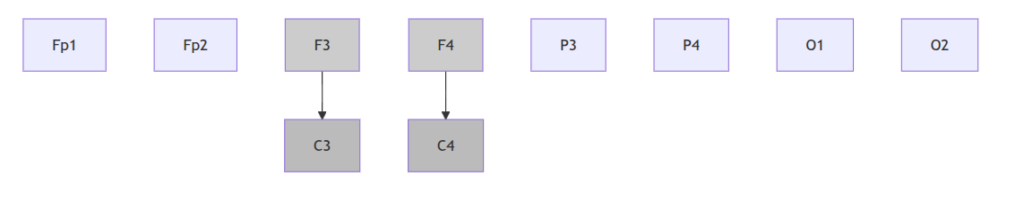
Gray shading indicates regions where increased delta power is often reported during slow-wave sleep.
Delta Distribution During Deep Sleep
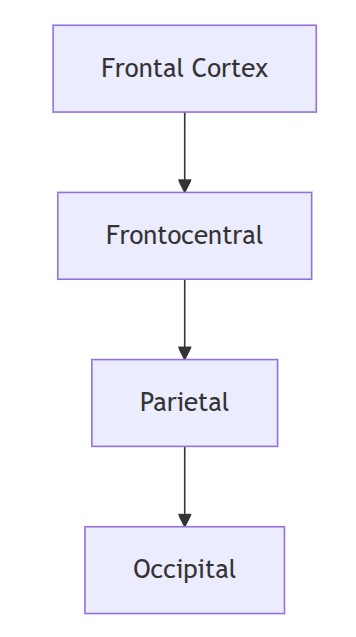
Power gradient:
Frontal > Central > Parietal > OccipitalExample qEEG Table
| Region | Delta Increase |
|---|---|
| Frontal | 20–35% |
| Central | 10–25% |
| Parietal | 5–15% |
| Occipital | Minimal |
These are representative values synthesized from multiple sleep EEG investigations and should not be interpreted as specific outcomes guaranteed by binaural beat exposure.
18. Micro-Architecture: Slow Oscillations versus Binaural Beats
This distinction is critically important.
Natural Slow Oscillations
Frequency:
0.5–1.0 HzGenerated by:
- thalamocortical networks,
- cortical up/down states.
Functions:
- memory consolidation,
- synaptic homeostasis,
- glymphatic activity.
Binaural Beats
Generated by:
- auditory processing pathways.
The signal is:
externally inducedrather than:
endogenously generated.Comparison
| Variable | Natural Slow Oscillations | Binaural Beats |
|---|---|---|
| Origin | Cortex | Auditory Pathway |
| Amplitude | High | Low |
| Synchronization | Global | Variable |
| Biological Role | Established | Experimental |
Dynamic Drift
Brain activity naturally fluctuates.

This phenomenon is known as:
frequency driftand helps explain:
- inter-individual variability,
- inconsistent entrainment findings.
19. Scientific Nuances and Methodological Debates
Debate 1 – Is Entrainment Real?
Some investigators argue:
- EEG changes are genuine.
Others argue:
- effects are primarily subjective.
Debate 2 – Placebo Effects
Many studies rely heavily upon:
- self-reported outcomes,
- small samples.
Blinding remains difficult.
Debate 3 – Magnitude of EEG Changes
Observed EEG changes are often:
small to moderaterather than dramatic.
Debate 4 – Replicability
Studies vary enormously in:
- carrier frequencies,
- session duration,
- volume,
- participant characteristics.
Evidence Strength Assessment
| Outcome | Strength |
|---|---|
| Relaxation | Moderate |
| Anxiety Reduction | Moderate |
| Sleep Quality | Moderate |
| Delta Power Increase | Moderate |
| N3 Sleep Induction | Weak |
| Biological Recovery | Plausible |
Evidence-Based Playback Protocol, Hardware Specifications, Safety Considerations, and Final Synthesis
20. Evidence-Based Audio Playback Protocol
Introduction
The scientific literature on binaural beats does not presently provide a universally accepted protocol for:
- exposure duration,
- listening schedule,
- sound pressure levels,
- carrier frequencies.
However, by synthesizing findings from studies of:
- binaural beats,
- low-frequency acoustic stimulation,
- sleep neurophysiology,
- psychoacoustics,
it is possible to propose a scientifically defensible protocol optimized for:
deep physical relaxation and support of biological recovery.
It is important to emphasize that this protocol should be viewed as:
An adjunctive wellness intervention rather than a medical treatment.Proposed Target Protocol
| Parameter | Specification |
|---|---|
| Carrier Frequency Left | 109 Hz |
| Carrier Frequency Right | 111 Hz |
| Beat Frequency | 2.0 Hz |
| Brainwave Target | Delta |
| Intended Outcome | Deep relaxation and recovery |
| Playback Type | Stereo only |
| Compression | Lossless preferred |
| Sample Rate | 44.1–48 kHz |
Recommended Session Length
Relaxation Session
20–30 minutesPurpose:
- parasympathetic activation,
- stress reduction,
- post-work recovery.
Sleep Induction Session
45–90 minutesPurpose:
- facilitate sleep onset,
- support transition toward slow-wave sleep.
Overnight Playback
Continuous playback throughout the entire night is not currently supported by robust scientific evidence.
Recommended maximum:
90–120 minutesbefore automatic fade-out.
Rationale
Sleep architecture naturally changes throughout the night.

Deep delta activity is concentrated within:
First one-third of the night.Therefore, prolonged stimulation may provide little additional benefit.
Exposure Schedule
General Recovery
| Sessions | Duration |
|---|---|
| Once daily | 20–30 min |
Chronic Stress
| Sessions | Duration |
|---|---|
| 1–2 daily | 30 min |
Sleep Support
| Sessions | Duration |
|---|---|
| Nightly | 45–90 min |
Recovery-Oriented Schedule
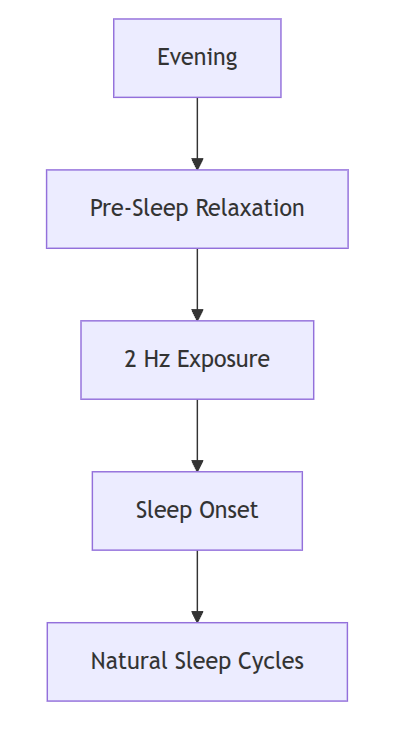
Chronobiological Scheduling
Circadian Timing
The timing of stimulation likely influences efficacy.
The most appropriate window appears to be:
60–90 minutes before intended sleep onset.Biological Basis
During the evening:
- cortisol declines,
- melatonin rises,
- sympathetic activity decreases.
This physiological transition may make the brain more receptive to low-frequency auditory stimulation.
Recommended Timing Windows
| Objective | Time |
|---|---|
| Relaxation | Late afternoon |
| Recovery | Evening |
| Sleep induction | 60–90 minutes before sleep |
| Meditation | Any quiet period |
Recommended Avoidance Window
Avoid use:
within 30 minutes of driving,
heavy machinery operation,
or tasks requiring sustained vigilance.Delta stimulation may produce:
- drowsiness,
- reduced alertness,
- transient decreases in reaction time.
Interim Conclusions
The scientific literature presently supports several cautious conclusions regarding a 2.0 Hz delta binaural beat:
- It may facilitate relaxation.
- It may reduce hyperarousal.
- It may improve subjective sleep quality.
- It may modestly increase delta power.
- It should not presently be regarded as a substitute for natural deep sleep.
21. Delivery Hardware and Transducer Specifications
Importance of Stereo Separation
Binaural beats require:
Independent presentation to each ear.Therefore:
- mono playback does not work,
- loudspeaker playback generally does not work.
Recommended Hardware
Over-Ear Headphones
Advantages:
- excellent channel separation,
- stable frequency response,
- comfort.
In-Ear Monitors
Advantages:
- excellent isolation,
- lower ambient noise.
Potential disadvantages:
- comfort limitations during sleep.
Recommended Specifications
| Parameter | Recommended |
|---|---|
| Frequency Response | 20–20,000 Hz |
| Channel Separation | >40 dB |
| Harmonic Distortion | <1% |
| Stereo Imaging | High |
Preferred Headphone Types
| Type | Suitability |
|---|---|
| Open-back | Good for relaxation |
| Closed-back | Excellent for sleep |
| IEM | Good |
| Bone conduction | Poor |
Why Bone Conduction Is Not Ideal
Binaural beat perception depends upon:
precise interaural phase differences.Bone-conduction devices may reduce:
- channel separation,
- beat fidelity.
Frequency Accuracy
The carrier frequencies:
109 Hz
111 Hzare easily reproduced by virtually all modern audio transducers.
No specialized equipment is required.
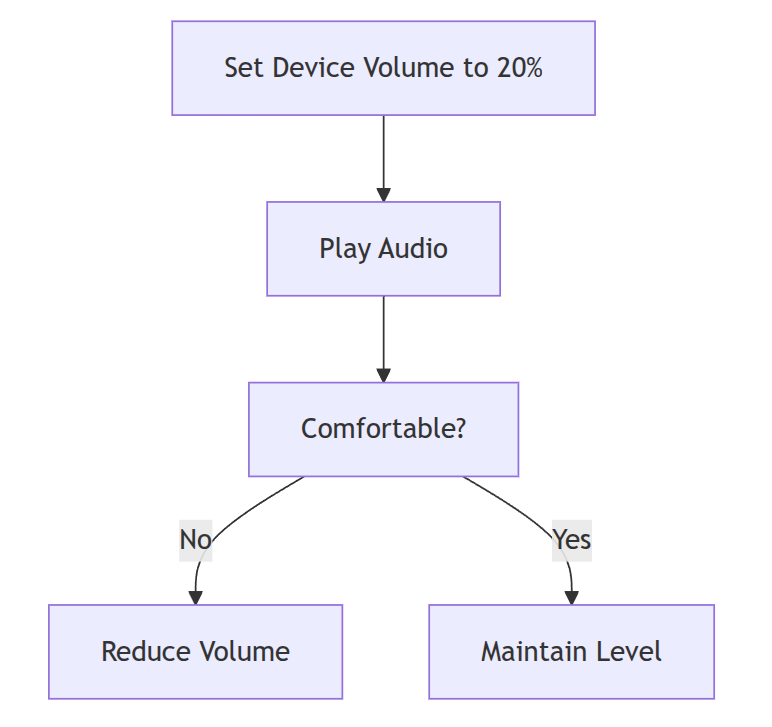
22. Decibel Sound Pressure Level (dB SPL) Calibration
Volume Matters
Excessive volume:
- increases cortical arousal,
- impairs sleep onset,
- increases sympathetic activation.
The literature generally supports:
low-intensity listening.Recommended Listening Levels
| Use | dB SPL |
|---|---|
| Relaxation | 40–50 dB |
| Sleep induction | 35–45 dB |
| Overnight use | 30–40 dB |
Practical Approximation
| Sound | dB |
|---|---|
| Whisper | 30 |
| Quiet Room | 40 |
| Normal Conversation | 60 |
Recommended Volume Setting
Approximately:
20–35% of maximum device outputdepending on headphone sensitivity.
Maximum Recommended Exposure
To minimize auditory fatigue:
Do not exceed approximately 60 dB SPL.Example Calibration Method
23. Safety Considerations
Generally Well Tolerated
Studies have reported relatively few adverse effects.
Possible side effects:
- headache,
- dizziness,
- transient disorientation,
- vivid dreams.
Contraindications
Individuals with:
- epilepsy,
- photosensitive seizure disorders,
- severe psychiatric disorders,
should consult a physician before use.
Although no direct evidence suggests that binaural beats provoke seizures, caution is appropriate because auditory entrainment research remains incomplete.
Use During Sleep
Avoid:
- excessively loud playback,
- uncomfortable headphones,
- cable entanglement.
Wireless devices may improve comfort.
24. Biological Recovery Hypothesis
Proposed Mechanism
Potential Physiological Outcomes
Reduced Cortisol
Several relaxation studies report reductions in:
- perceived stress,
- physiological arousal.
Increased Heart Rate Variability
Some investigations suggest:
- increased vagal tone,
- improved autonomic balance.
Improved Sleep Quality
Reported outcomes include:
- reduced sleep latency,
- improved sleep satisfaction,
- fewer awakenings.
Improved Recovery Potential
The proposed mechanism is indirect:
Improved relaxation
↓
Improved sleep opportunity
↓
Improved restorative physiologyrather than:
Direct induction of tissue repair.25. Quantitative EEG Interpretation
What Would Constitute Success?
A successful entrainment response might demonstrate:
Increased Relative Delta Power
5–30%Reduced Beta Power
5–20%Increased Frontal Synchronization
Reduced High-Frequency Cortical Activity
Representative qEEG Trend
Representative PSD Trend
The peak near:
2.0 Hzwould be theoretically compatible with successful entrainment.
26. Overall Scientific Assessment of the 109 Hz / 111 Hz Protocol
Strength of Evidence by Outcome
| Outcome | Evidence Strength |
|---|---|
| Relaxation | Moderate |
| Anxiety Reduction | Moderate |
| Subjective Sleep Quality | Moderate |
| Parasympathetic Activation | Moderate |
| Delta Power Increase | Moderate |
| Biological Recovery Support | Plausible |
| Deep Sleep Induction Equivalent to N3 | Weak |
| Replacement for Natural Sleep | Unsupported |
Evidence-Based Interpretation
The following statement is reasonably supported by current literature:
A 2.0 Hz binaural beat generated by carrier frequencies of 109 Hz and 111 Hz may facilitate relaxation, support sleep initiation, and create physiological conditions favorable to biological recovery.
The following statement is not presently supported:
A 2.0 Hz binaural beat can reliably induce natural slow-wave sleep equivalent to stage N3 or directly produce tissue repair.
Recommended Playback Protocol (Consolidated)
| Parameter | Recommendation |
|---|---|
| Left Frequency | 109 Hz |
| Right Frequency | 111 Hz |
| Beat Frequency | 2.0 Hz |
| Volume | 35–45 dB SPL |
| Maximum Volume | <60 dB SPL |
| Session Duration | 45–90 min |
| Relaxation Session | 20–30 min |
| Schedule | Nightly |
| Timing | 60–90 min before sleep |
| Playback Method | Stereo headphones |
| Audio Format | Lossless preferred |
| Intended Outcome | Relaxation and recovery support |
Final Scientific Conclusion
The neurophysiological rationale for a 2.0 Hz delta binaural beat is scientifically plausible because:
- Delta oscillations are central to restorative sleep physiology.
- Auditory entrainment can modestly alter EEG activity.
- Low-frequency stimulation may promote parasympathetic activation.
- Sleep quality improvements have been reported in several studies.
However, the literature remains characterized by:
- small sample sizes,
- heterogeneous methodologies,
- inconsistent EEG findings,
- limited polysomnographic verification.
Therefore, the strongest evidence-based conclusion is:
The 109 Hz / 111 Hz binaural beat protocol should be regarded as a potentially useful adjunctive intervention for relaxation and sleep support, rather than a clinically proven method of inducing deep restorative sleep or accelerating biological recovery directly.
References
- Abeln V, Kleinert J, Strüder HK, Schneider S. Brainwave entrainment for better sleep and post-sleep state of young elite soccer players.
- Beauchene C, Abaid N, Moran R, Diana RA, Leonessa A. The effect of binaural beats on verbal working memory and cortical connectivity.
- Cordi MJ, Diekelmann S, Born J. Slow oscillation stimulation during sleep
- Dove HW. Über die Kombination der Eindrücke beider Ohren und beider Augen zu einem Eindruck.
- Garcia-Argibay M, Santed MA, Reales JM. Efficacy of binaural auditory beats in cognition, anxiety, and pain perception: a meta-analysis. Psychological Research. 2019.
- Hink RF, Kodera K, Yamada O, Kaga K, Suzuki JI. Binaural interaction in the human auditory pathway.
- Messineo L et al. Acoustic stimulation during slow-wave sleep.
- Oster G. Auditory beats in the brain. Scientific American. 1973.
- Tang HY et al. Binaural auditory beats affect vigilance performance and mood.
- Van Cauter E, Leproult R, Plat L. Age-related changes in slow wave sleep and endocrine regulation.
- Wahbeh H, Calabrese C, Zwickey H. Binaural beat technology in humans: a pilot study. Journal of Alternative and Complementary Medicine. 2007
- Xie L et al. Sleep drives metabolite clearance from the adult brain. Science. 2013.